9400 WEST HIGGINS ROAD SUITE 215 ROSEMONT IL 600184261
042017 ASSOCIATION OF PROFESSIONAL CHAPLAINS 2800 WEST HIGGINS ROAD9400 WEST HIGGINS ROAD SUITE 215 ROSEMONT IL 600184261
© 1998 IRENE HIGGINSON PUBLISHED HERE WITH PERMISSION THE
Barbara j Grosz Higgins Professor of Natural Sciences tel
C OLEGIO AMBROSIO O`HIGGINS – DEPARTAMENTO DE CIENCIAS GUIA
COLEGIO AMBROSIO O’HIGGINS VALLENAR EXPERIMENTO ALEATORIO Y ESPACIO MUESTRAL
Orthopaedic Research and Education Foundation
|
|
9400 West Higgins Road, Suite 215 Rosemont, IL 60018-4261 Follow Instructions Carefully
|
||||||||
|
1. TITLE OF PROJECT |
|||||||||
|
2. Principal Investigator Information (See Page AA-1 For Co-Principal Investigator Information) |
|||||||||
|
2a. Name: (Last, First, Middle)
|
2b. Degrees: |
2c: NATIONAL PROVIDER IDENTIFICATION NO. (if applicable): |
|||||||
|
2d. Position Title:
|
2e. BUSINESS Address (Street, City, State, Zip)
|
||||||||
|
2f. DEPARTMENT, SERVICE, LABORATORY OR EQUIVALENT |
|||||||||
|
2g. TELEPHONE AND FAX (Area code, number, extension) Tel.: Fax: |
2h. EMAIL ADDRESS (required) 2I. ALTERNATE EMAIL: |
||||||||
|
3. Human Subjects: YES NO PENDING
|
3a. If “YES”, Exemption #: Or IRB Approval Date: Full IRB Expedited Review |
||||||||
|
5. Dates Of Proposed Period Of Support:
|
6. Costs Requested for Each Year: - 2 or 3 Years YEAR 1 YEAR 2 YEAR 3
|
7. Total Costs Requested:
|
|||||||
|
8a. Applicant Organization: 8b. Address Name: |
|||||||||
|
9a. Department Chair Name: Business Address: City, State, Zip: Phone: Fax: E-mail (required): |
10. AUTHORIZED INSTITUIONAL Official Signing for Applicant Organization (Administrative Official to be notified if Award is Made) Name: Title: Business Address: City, State, Zip: Phone: Fax: E-mail (required): |
||||||||
|
9b. SIGNATURE: |
9c. DATE: |
||||||||
|
11. Principal Investigator Assurance: I certify that the statements herein are true, complete and accurate to the best of my knowledge. I am aware that any false, fictitious, or fraudulent statements or claims may subject me to administrative penalties. I agree to accept responsibility for the scientific conduct of the project and to provide the required progress reports if a grant is awarded as a result of this application |
Signature of PI Named in 2a: (In ink. “Per” signature not acceptable.) |
Date: |
|||||||
|
12. Applicant Organization Certification and Acceptance: I certify that the statements herein are true, complete and accurate to the best of my knowledge, and accept the obligation to comply with OREF terms and conditions if a grant is awarded as a result of this application. I am aware that any false, fictitious, or fraudulent statements or claims may subject me to administrative penalties. |
Signature of Official Named in 10: (In ink. “Per” signature not acceptable.) |
Date: |
|||||||

|
13. CO-Principal Investigator Information |
|||
|
13a. Name: (Last, First, Middle)
|
13b. Degrees: |
13c. NATIONAL PROVIDED IDENTIFICATION NO. (if applicable): |
|
|
13d. Position Title:
|
13e. BUSINESS Address (Street, City, State, Zip)
|
||
|
13f. DEPARTMENT, SERVICE, LABORATORY OR EQUIVALENT |
|||
|
13g. TELEPHONE AND FAX (Area code, number, extension) Tel.: Fax: |
13h. EMAIL ADDRESS (required): |
||
|
13i. SIGNATURE OF CO-PRINCIPAL INVESTIGATOR |
|||
|
14. FINANCIAL OFFICER INFORMATION |
|||
|
14a. AUTHORIZED FINANCIAL OFFICER Name: Phone: Title: Fax: Business Address: E-mail (required): City, State, Zip: |
|||
|
14b. FINANCIAL OFFICER SIGNATURE: |
|||
|
PAYMENT INFORMATION Payee For Check: Mail check to (required if person is not financial officer listed above): Address For Check: City, State, Zip: |
|||
|
15. ADDITIONAL INVESTIGATOR INFORMATION |
|||
|
15. NAME AND SIGNATURE OF ADDITIONAL INVESTIGATORS (If Applicable) 1). NAME: SIGNATURE:
2). NAME: SIGNATURE: |
|||
|
16. ALTERNATE CONTACT INFORMATION |
|||
|
PROVIDE THE NAME AND CONTACT INFORMATION FOR AN ALTERNATE CONTACT — this is the person OREF should contact (e.g., administrative assistant, research assistant, etc.) if there is a question regarding the application and the PI cannot be reached. Must not be Co-PI or additional investigators.
NAME: PHONE: E-MAIL (required):
|
|||
Face Page Form page 1
COLEGIO AMBROSIO O`HIGGINS – DEPARTAMENTO DE CIENCIAS N ELECTRÓNICA
Higgins-Lockie%20JRS%20Article%20%285th%20draft%29
LONGUETHIGGINS EARLY CAREER RESEARCHER PRIZE NOMINATION FORM 2015 THE
Tags: higgins, rosemont, suite, 600184261
- 6 BALANCE ENERGÉTICO DE LA VACA LECHERA DURANTE EL
- VALUATION STRATEGIES (WG&L) GOING CONCERN PROPERTY TRANSACTIONS THE NECESSITY
- EVROPSKI PRAVNI CENTER KOMENSKEGA ULICA 36 1000 LJUBLJANA PE
- TÍTULODENOMINACIÓN HABLAR Y SIGNAR UNA APP PARA LA IMPLEMENTACIÓN
- ………………………………………………… IMIĘ I NAZWISKO JEDNOSTKA ………………………………… IMIONA RODZICÓW
- WORKING TITLE SHARKS MORE THAN JAWS MAIN ISSUES
- SUFFOLK COASTAL DISTRICT COUNCIL APPLICATION FOR BEACH HUT OWNER’S
- EL MOVIMIENTO CONCEPTOS BÁSICOS MOVIMIENTO RECTILINEO Y UNIFORME A
- CONFUSION FOR THREE JO LLOYD WEDNESDAY 26 –
- NOTE THESE NOTES MUST BE INCLUDED AS PART OF
- WEATHER PROTECTION GRILLE ALAS SPECIFICATION TEXTS EXTERNAL AIR INTAKE
- CERERE DE ÎNSCRIERE LA EXAMENUL DE ABSOLVIRE 2021 AL
- ZÁPIS Z JEDNÁNÍ VALNÉ HROMADY OS PŘÁTEL GVP KONANÉ
- ………………………………………………… LUBLIN ……………………… (STUDENT’S NAME AND SURNAME [FAMILY NAME])
- AJUNTAMENT D’OLOST PL MAJOR 1 08516 – OLOST TELF
- XML DA NFE? OBRIGAÇÕES LEGAIS NOTAS FISCAIS ELETRÔNICAS MERCADORIAS
- INFORMATIVO 022018 DO ESTUDO DE VIABILIDADE PARA INSTITUIÇÃO
- 2 MEMORÁNDUM DE ENTENDIMIENTO – GMPCS SEGUNDA
- MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY CONSULTS 800 815
- B ELFAST METROPOLITAN COLLEGE RECORDS MANAGEMENT POLICY 1 SUMMARY
- CASE MANAGEMENT MEMORANDUM CASE MANAGEMENT MEMORANDUM S 56 CRIMINAL
- RECTÁNGULO 7 AMPARO DIRECTO EN REVISIÓN 62772015 AMPARO DIRECTO
- PROY DE LEY MEDIANTE EL CUAL LA SECCIÓN DE
- DINAMIZACIÓN DE LA BIBLIOTECA ESCOLAR ESTE DOCUMENTO OFRECE UN
- 6 TO 12 MONTHS BEFORE THE HEALTH FAIR
- ADS INVESTIGACIÓN EN INTERNET NORMALIZACIÓN DE BASES DE DATOS
- LAST REVIEWREVISION DATE BY MAINE DOE AUGUST 2017 GRAPHIC
- PROGRAMA FUNDACIÓN SEPI – IBERIA LAE 2009 BASES DE
- ANNEX 3 3 YEARS 8 MONTHS 20 DAYS CAST
- HTTPWWWDRAKEEDUARTSCIDRAKEPROGREVAPRGUIDEHTML CLARIFICATION OF PROGRAM DEFINITION 1 EVERY PROGRAM THAT
TABLE 2 SUMMARY OF INFORMATION ON POSSIBLE ALTERNATIVE EXPLANATIONS
CONSTANT FLUX MEDIA AND COMMUNICATION FROM TELEGRAPH TO TWITTER
RELIGIOUSLY AFFILIATED ORGANIZATIONS AND THE OPPORTUNITIES AND CHALLENGES OF
 OPĆINSKA NAČELNICA O D L U K E OPĆINSKE
OPĆINSKA NAČELNICA O D L U K E OPĆINSKE FORMULARIO DE INGRESO NOTIFICACIÓN DE NORMATIVA VIGENTE UNT DEPENDENCIA
FORMULARIO DE INGRESO NOTIFICACIÓN DE NORMATIVA VIGENTE UNT DEPENDENCIA INFORME DE PARTICIPACIÓN CIUDADANA Y RENDICIÓN DE CUENTAS DICIEMBRE
INFORME DE PARTICIPACIÓN CIUDADANA Y RENDICIÓN DE CUENTAS DICIEMBRE STRONGER SUSTAINABLE CLUBS FUNDING FOR YOUR CLUB – SOURCES
STRONGER SUSTAINABLE CLUBS FUNDING FOR YOUR CLUB – SOURCES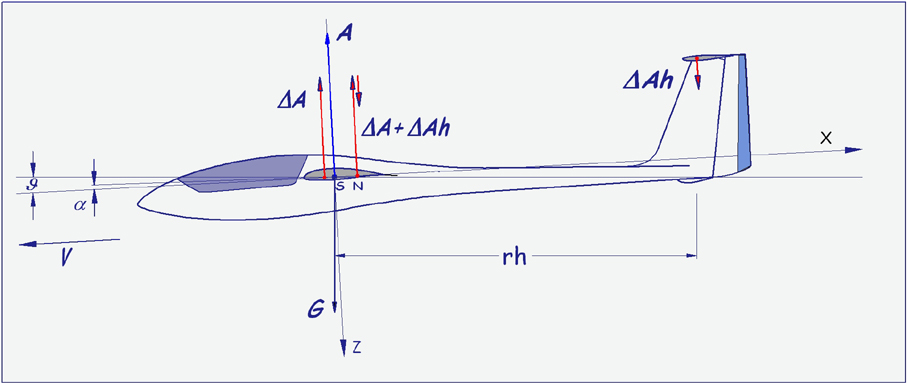 135 DR HELMUT QUABECK FINKENWEG 39 64832 BABENHAUSEN GERMANY
135 DR HELMUT QUABECK FINKENWEG 39 64832 BABENHAUSEN GERMANY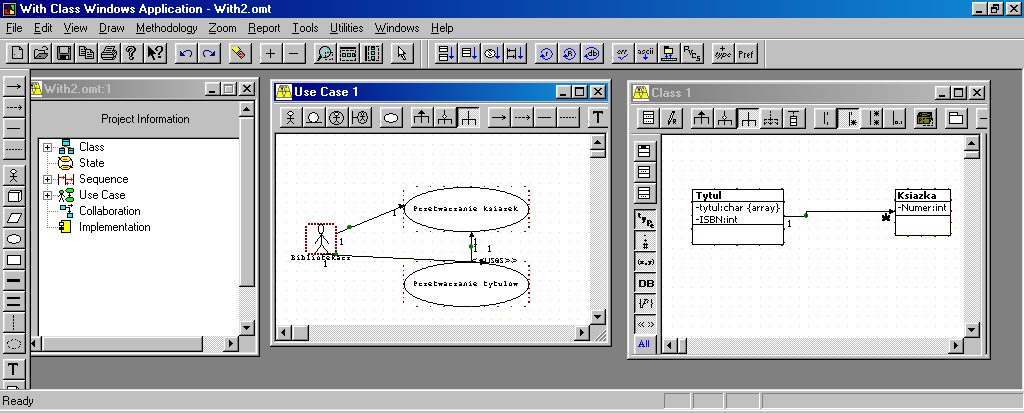 WYKŁAD 2 POWIĄZANIA MIĘDZY KLASAMI – PROJEKT I IMPLEMENTACJA
WYKŁAD 2 POWIĄZANIA MIĘDZY KLASAMI – PROJEKT I IMPLEMENTACJASMJERNICE ZA POPUNJAVANJE ZAJEDNIČKOG ULAZNOG DOKUMENTAZUD (COMMON ENTRY DOCUMENT
SPEECH BY PROFESSOR CHONG CHI TAT NUS DEPUTY PRESIDENT
 LA TRISTEZA Y SU FUNCIÓN HOMEOSTÁTICA SE ME OCURRIÓ
LA TRISTEZA Y SU FUNCIÓN HOMEOSTÁTICA SE ME OCURRIÓDEVELOPABLE SURFACES IN MAP PROJECTIONS – A PANDEMIC MILJENKO
SECRETARÌA DE EDUCACIÒN MUNICIPAL INSTITUCIÓN EDUCATIVA NORMAL SUPERIOR DE
MAINE EDRS PARTICIPANTS AS OF JULY 30 2010 MUNICIPAL
 FACULTAD HUMANIDADES GUÍA DE TRABAJO PRÁCTICO MÉTODOS Y TÉCNICAS
FACULTAD HUMANIDADES GUÍA DE TRABAJO PRÁCTICO MÉTODOS Y TÉCNICAS PRZEJDŹ DO GŁÓWNEGO MENU PRZEJDŹ DO TREŚCI HAMBURGERMENU
PRZEJDŹ DO GŁÓWNEGO MENU PRZEJDŹ DO TREŚCI HAMBURGERMENU REGULAMIN SZKOŁY PODSTAWOWEJ INTEGRACYJNEJ NR 339 IM RAOULA WALLENBERGA
 PODÁNÍ NA ELEKTRONICKÉM NOSIČI (EMAIL FLASH DISK ATD) PŘÍLOHA
PODÁNÍ NA ELEKTRONICKÉM NOSIČI (EMAIL FLASH DISK ATD) PŘÍLOHA POWIATOWY URZĄD PRACY W KALISZU 62800 KALISZ UL STASZICA
POWIATOWY URZĄD PRACY W KALISZU 62800 KALISZ UL STASZICA
