NEGLECT OF REFUGEE PARTICIPATION BY MARIE THERES BENNER AREE
9 QUINTON’S NEGLECTED ARGUMENT FOR SCIENTIFIC REALISM SILVIOADMINISTRATIVELY RESTRICTED [TYPE TEXT] SUSPECTED CHILD ABUSENEGLECT REPORT (SCAN)
CHILD ABUSE AND NEGLECT POLICY – MANAGEMENT OF PAGE
Child%20Abuse%20It%20Matters%20You%20%20What%20is%20Neglect
DYFFRYN NANTLLE – A LANDSCAPE OF NEGLECT NANTLLE
IDENTIFICATION OF ATTRACTIVE DRUG TARGETS IN NEGLECTEDDISEASE PATHOGENS USING
How participative is NGO refugee aid on the Thai-Myanmar (Burmese) Border
Neglect of refugee participation
by Marie Theres Benner, Aree Muangsookjarouen, Egbert Sondorp and Joy Townsend
The participation of affected populations in planning or implementation of humanitarian aid in conflict or post-conflict situations has too often been neglected.
There has been a notable progression to systematic aid dependency among the Myanmar refugees living in nine camps along the Thai-Myanmar border. Refugee participation shifted from self-reliance for shelter and food to the current situation in which the refugees have become fully dependent on the international community for their living in Thailand, tempered by partial self-management of their own health care, education services and food distribution.
The first documented Burmese refugees arrived in Thailand in 1976, scattering to several small so-called ‘displaced persons camps’ along the Salween river that forms the border. Camps held between 300 and 2,000 refugees, who made their living by trading goods. At first, aid agencies provided essential drugs, vaccines, basic health-care training and services, as well as certain basic commodities. During the mid-eighties the refugees continued to be able to earn their own income, and retained control over their housing and most of their food supply. They were able to plant their paddy fields and vegetables across the border in Myanmar and to raise domestic livestock in the camps. Assistance was minimal, and mainly organised and managed by the refugees themselves.
The large increase in the number of refugees entering Thailand after 1988 and again in 1994-95 resulted in a more systematic ‘top-down’ approach, providing health care, shelter and nutrition, with planning and implementation mainly through NGOs, who were requested by the Royal Thai Government to increase their services in order to avoid outbreaks of disease. These services included implementation of a health surveillance system, provision of essential drugs, immunisation against communicable diseases, treatment of the most problematic diseases such as diarrhoea, malaria and tuberculosis, laboratory training and services, training of refugees in health-care services and management, water supply and sanitation. NGOs also needed to provide food supplies and shelter as the refugees were no longer allowed to organise their own. The level of humanitarian assistance was not allowed to exceed the living standards of the Thai host communities, in order to avoid inequalities.
There was a consolidation of the camps in the late 1990s, resulting in larger camp settlements with up to 45,000 refugees in the largest camp. The number of camps was reduced from 29 in 1994 to nine camps by 2007. Additional stringent movement restrictions set by the host government resulted in increased confinement in the camps with limited work and educational opportunities, which has led to almost complete dependence on aid over the last five years. Income was and is still only possible for the refugees working with one of the 19 aid agencies providing humanitarian assistance, or from daily labour work in the camp. Although many refugees have been trained with support from the Royal Thai Government, donors, local and international and NGOs in aspects of health-care management, education, food distribution and camp management, very few refugees are now able to earn an income working outside this structure. Over the years some small refugee community-based groups have been established and supported, including the Karen’s Women Organisation and the Karen Women’s Education Group, which are mainly engaged in women’s and adolescents’ health and education, and which operate more or less independently of the international NGOs. They depend on donor commitment and availability of funds as well as on the international NGOs’ philosophy regarding participation of those affected by conflict.
This refugee population has therefore moved from relative independence in the early years to an almost total dependency on aid. Refugee ‘participation’ has been reduced to providing staff for health and education services and food distribution – to the administration of activities rather than the design and planning of programmes. If this is to be avoided here, and in other protracted refugee crises, the international community and host governments need to pay far greater attention to:
involving refugees early on in the planning and designing of programmes
providing work opportunities to ensure self-sufficiency and reduce aid dependency
ensuring that aid supports the integration, rather than isolation, of refugees, with an emphasis on building trust, synergy and good relationships between refugee and host communities.
Marie Theres Benner ([email protected]) is a Senior Health Coordinator for Malteser International (www.malteser.de/61.Malteser_International). Aree Muangsookjarouen ([email protected]) works on Burmese migrant and refugee health issues with the World Health Organisation in Bangkok. Egbert Sondorp ([email protected]) is a Senior Lecturer on Conflict and Health, and Joy Townsend ([email protected]) is Emeritus Professor of Primary Health Care, both at the London School of Hygiene and Tropical Medicine (www.lshtm.ac.uk). The views expressed in this article do not necessarily reflect those of the organisations.
MULTIAGENCY NEGLECT STRATEGY 1 INTRODUCTION 11 ‘THE POSSIBILITY THAT
NEGLECT OF REFUGEE PARTICIPATION BY MARIE THERES BENNER AREE
NEWAYGO COUNTY PREVENTION OF CHILD ABUSE AND NEGLECT (PCA)
Tags: benner ([email protected]), benner, theres, refugee, marie, participation, neglect
- HOMESCHOOLED STUDENTS A PPLICATION FOR HOMESCHOOLED STUDENTS TO ENTER
- TIVERTON COOPERATIVE LEARNING PARTNERSHIP BAMPTON CHURCH OF ENGLAND PRIMARY
- PRESENTACIÓN DE UNA MATRIZ PROPUESTA PARA LA GENERACIÓN DE
- DOMAINE VISTALBA SA TFN SALA B DEL 122005 IMPUESTO
- FORMULARE ȘI MODELE CONŢINE FORMULARELE DESTINATE PE DE
- STATYSTYKA ŹRÓDŁEM WIEDZY SPRAWOZDANIE ZE SPOTKANIA REGIONALNEGO ŚRODOWISKA
- MODELO PLAN ESTRATÉGICO DE VOLUNTARIADO LOCAL MODELO PLAN ESTRATÉGICO
- AR TESS INSTRUCTIONAL SPECIALIST EVALUATION FORM INSTRUCTIONAL SPECIALIST EVALUATOR
- Department of Environmental Protection Chris Christie Division of Land
- APEC NON‑BINDING INVESTMENT PRINCIPLES JAKARTA NOVEMBER 1994 IN THE
- WASTEWATER DISCHARGE PERMIT APPLICATION THIS APPLICATION IS REQUIRED IN
- DENUMIREA PRINCIPALELOR DOTĂRI ECHIPAMENTE MIJLOACE DE TRANSPORT ETC NECESARE
- MINISTARSTVO POLJOPRIVREDE RIBARSTVA I RURALNOG RAZVOJA 1993 NA TEMELJU
- SERVIÇO PÚBLICO FEDERAL MINISTÉRIO DA EDUCAÇÃO UNIVERSIDADE FEDERAL DO
- SENTERETS TJENESTETILBUD – UT OVER OPPFØLGING AV SENTERETS BEBOERE
- COMMUNITY PLANNING PARTNERSHIP WELCOME PACK ALL YOU
- OBJAŚNIENIA DO FORMULARZA G – 104 (OB) 2003
- ENDUSER LICENSE AGREEMENT PLEASE READ CAREFULLY BEFORE USING THIS
- APLICACIONES DE LA DERIVADA (CONTINUACIÓN) 2 PUNTOS MÁXIMOS MÍNIMOS
- NOTIFICAION IN EXERCISE OF THE POWERS CONFERRED BY CLAUSE
- INTERNATIONAL EXPECT GROUP MEETING INDIGENOUS CHILDREN AND YOUTH IN
- 9 (UNOFFICIAL TRANSLATION) CODIFIED UP TO NO4 AS OF
- OUTLINE FOR A REVIEW PAPER TO THE RAMSAR STRP
- DER ERFOLGREICHE WEG ZUM ABITUR … MÜNDLICHE PRÜFUNG –
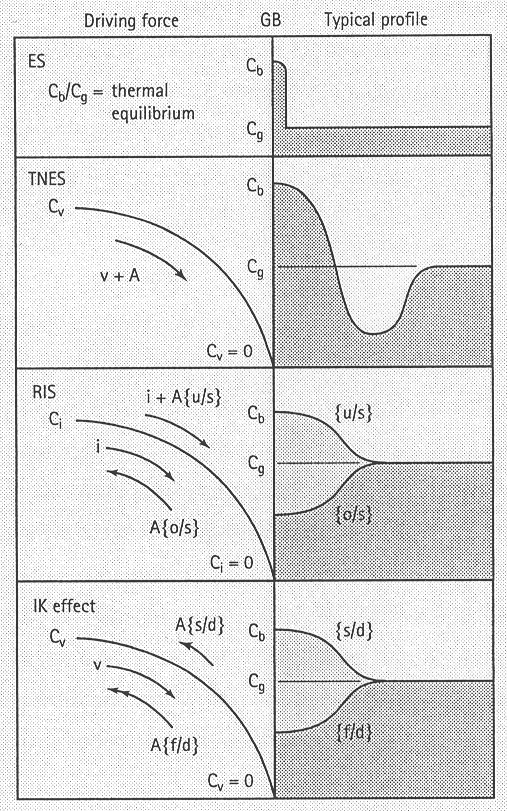
- INFLUENCE OF TRANSPORT PARAMETERS AND CHEMICAL PROPERTIES OF THE
- LISTA DE PRODUCTOS NO PROBADOS EN ANIMALES CADA
- PAGE 5 OCTOBER 2010 POWERTRAIN WIDE CHOICE OF FUELEFFICIENT
- HTTPWWWFILASTROCCHEITCONTEMPOPLAYCOBONITATESTOSPASP LA CASA BONITA JOSEFINA URDANETA UN BUEN DÍA
- ACTIVITIES FOR AUTHOR IN YOU FEATURING JOSÉ ARUEGO ACTIVITY
- ACTA DEL CONSEJO DE SALUD Y CONSUMO CELEBRADO EL
SCENARIUSZ SYTUACJI EDUKACYJNEJ Z ZAKRESU POZNAWANIA PRZYRODY I POJĘĆ
VIERNES 6 DE FEBRERO DE 2009 DIARIO OFICIAL (SEGUNDA
RESUM DE LA CONFERÈNCIA JORNADES DE CULTURA CATALANA A
CROATIA (UPDATE 26 JAN 06) OP 2 BIOLOGICAL
TRANSPORTING EQUIPMENT FOR RESEARCH COLLABORATIONS FACULTY MEMBERS WHO INTEND
 MODELLING OF WELD MICROSTRUCTURES IN FERRITIC AND AUSTENITIC STEELS
MODELLING OF WELD MICROSTRUCTURES IN FERRITIC AND AUSTENITIC STEELS key Account Manager – ict Ovum has an Exciting
key Account Manager – ict Ovum has an Exciting ARTÍCULO TÉCNICO ETIQUETADO Y USO DE DECLARACIONES DE PROPIEDADES
ARTÍCULO TÉCNICO ETIQUETADO Y USO DE DECLARACIONES DE PROPIEDADESGEORGIA VICTIMS ASSISTANCE ACADEMY JOB RETENTION AND COMPETENCY FOLLOWUP
CHAPTER 2 MULTIPLE CHOICE QUESTIONS A BROKERAGE ACCOUNT IN
INSTRUCTIONS WITH YOUR MOUSE CURSOR CLICK ONCE IN THE
 ANIMALS IN DISASTERSMODULE A UNIT 3 ANIMALS IN DISASTERS
ANIMALS IN DISASTERSMODULE A UNIT 3 ANIMALS IN DISASTERSKOMMUNALT PSYKISK HELSETILBUD 1 FORMÅLET MED TJENESTEN PSYKISK HELSEARBEID
 POWERPLUSWATERMARKOBJECT1032529861 STANDARDS FOR CITIZEN SCIENCE DATING 10TH NOVEMBER 2015
POWERPLUSWATERMARKOBJECT1032529861 STANDARDS FOR CITIZEN SCIENCE DATING 10TH NOVEMBER 2015KOMENTÁŘ K OBECNĚ ZÁVAZNÉ VYHLÁŠCE STATUTÁRNÍHO MĚSTA LIBEREC Č
NÁVRH MINISTERSTVA VNITRA POSTOUPENÝ ELEKTRONICKOU POŠTOU 25 LEDNA 2001
⑨防災女子【BOSAI JYOSHI】 PHÒNG TAI HỌA CHO CÁC EM NỮ
 TEACHING ABOUT SENTENCES SUBJECT KNOWLEDGE FOR TEACHERS’ REFERENCE
TEACHING ABOUT SENTENCES SUBJECT KNOWLEDGE FOR TEACHERS’ REFERENCE REPÚBLICA DE VENEZUELA CONTRALORÍA GENERAL DE LA REPÚBLICA
FEMINIST THEORY FOR HISTORIANS LEORA AUSLANDER WEDNESDAYS 300600 OFFICE
