ACKNOWLEDGMENT OF RECEIPT OF NOTICE OF PRIVACY PRACTICES (ELECTRONIC
ACKNOWLEDGMENT LETTER [LETTERHEAD OF BIDDER INCLUDING FULL POSTAL ADDRESSACKNOWLEDGMENT OF RECEIPT FOR COMPANYISSUED PROPERTY YOU MAY BE
ACKNOWLEDGMENT OF RECEIPT OF NOTICE OF PRIVACY PRACTICES (ELECTRONIC
ACKNOWLEDGMENT OF RECEIPT OF REQUEST
ACKNOWLEDGMENT OF RESPONSIBILITIES OF CLIENT AND PERSON LEGALLY RESPONSIBLE
ACKNOWLEDGMENT OF RISKS AND RELEASE OF RESPONSIBILITY OFFICE
Acknowledgment of Receipt of Notice of Privacy
Acknowledgment of Receipt of Notice of Privacy Practices
(Electronic Version)
PRIVACY POLICIES AND PROCEDURES
This Notice of Privacy Practices is made available to you via our website and/or at your request. Please fill out the document and return to:
Connecticut Neurodevelopmental Services
134 Grandview Avenue, Suite# 208
Waterbury, CT 06708
Fax# (203) 755-3057
I, ________________________________________have been offered a copy of
Connecticut Neurodevelopmental Services’ “Notice of Privacy Practices”. This notice describes in detail how my Protected Health Information (PHI) may be used or disclosed by Connecticut Neurodevelopmental Services according to HIPAA regulations and further describes my rights under HIPAA.
Please check one box below:
I have been offered a copy of the Notice of Privacy Practices and acknowledge I have received a copy.
I have been offered a copy of the Notice of Privacy Practices and am DECLINING to accept a copy.
Your signature below documents that you have been offered the Notice of Privacy Practices.
______________________________________________ __________________
Signature of Patient Date
______________________________________________ __________________
Printed name of authorized representative Date
______________________________________________ ________________________
Signature of authorized representative Relationship to Patient
Patient or authorized representative refused to sign this acknowledgement. _____________________ Printed name of CNS employee
Implemented: April 14, 2003
ACKNOWLEDGMENT OF SERVICE FORM 6 FAMILY COURT RULES
BELOW IS THE REQUIRED ACKNOWLEDGMENT FOR DEEDS STATE OF
CITY OF MELBOURNE 2018 BUSINESS MISSION TO JAPAN ACKNOWLEDGMENT
Tags: (electronic version), (electronic, practices, acknowledgment, receipt, notice, privacy
- COMMON GROUND A CROSSCULTURAL SELFDIRECTED LEARNER’S INTERNET GUIDE INDIVIDUAL
- PABLO DE SANTIS EL ENIGMA DE PARÍS TÍTULO
- TREŚĆ POZ SPIS TREŚCI DZIENNIKA URZĘDOWEGO WOJEWÓDZTWA ŁÓDZKIEGO NR
- SUESOLUCION NO ADOAF–02899 9 DE MARZO DE 1999
- REPUBLICA DE COLOMBIA RAMA JUDICIAL DEL PODER PÚBLICO
- VALORES EN LA FRONTERA EN DOS PUNTOS EL PROBLEMA
- FICHA DE LIBRO NOMBRE Y APELLIDOS NIF DIRECCIÓN CÓDIGO
- MARIANA FERRER VALENTINI RAFAEL SOTOMAYOR 953 SANTIAGO 963543837 MFERRERVALENTINIGMAILCOM
- ASPECTO FÍSICO DE LA REPÚBLICA ARGENTINA Y CARACTERES HÁBITOS
- VISUALIZANDO LA MÚSICA LA IMAGEN EN LA CANCIÓN LA
- FACT SHEET OFFICE OF THE HIGH COMMISSIONER FOR HUMAN
- THE DIFFERENCE BETWEEN BUTTER AND MARGARINE? BOTH HAVE THE
- UNIVERSITY OF WYOMING COLLEGE OF ARTS & SCIENCES REQUIREMENTS
- ¿PADECE USTED DE HIPERTENSIÓN? ¿TIENE LA ESPERANZA DE ALIVIAR
- PRYMASOSTWO W POLSCE – GENEZA I ZNACZENIE BERNADETA KRUSZYK
- EVIDENCE PSŮ BEZ PP ČESKÝ KYNOLOGICKÝ SVAZ PROVÁDÍ REGISTRACI
- MORSKA SŁUŻBA POSZUKIWANIA I RATOWNICTWA W GDYNI KLAUZULA ZGODY
- RULE INHERITANCE IN OBJECTBASED IMAGE CLASSIFICATION FOR URBAN LAND
- THE LARGE HADRON RAP – VELKÝ HADRONOVÝ RAP (KATE
- PREPARING A VOICE SCALE LAMINATE THE VOICE SCALE
- PRESS RELEASE BRITISH MUSEUM INTERNATIONAL EXHIBITIONS THE BRITISH MUSEUM
- CENTRO SPORTIVO ITALIANO COMITATO DI CARPI VIA PERUZZI 22
- T WINKLES NURSERY WINTER MENU WEEK 1 MONDAY TUESDAY
- ORGANIZATIONAL CULTURE IMPACT ON INFORMATION SYSTEMS SUCCESS ISMAIL M
- TABLA Nº 2 TABLA DE DESCOMPRENSION NORMAL CON AIRE
- GEBIRGSTÄLER EINFÜHRUNG DIE VORARLBERGER GEBIRGSTÄLER ZEIGEN EINE REICHE
- MANAGING CONFLICTS OF INTEREST BETWEEN DOCTORS AND ROS IN
- 22ND ANNUAL EFVET INTERNATIONAL CONFERENCE THE COLLEGE THAT WORKS!!!
- FESTIVALS PROGRAMMATION 2017 MUSIQUE SAISON 20162017 DE CONCERTS
- 5 PATVIRTINTA GENERALINIO DIREKTORIAUS 2016 M SAUSIO 26 D
 OLGA VLASOVA FREELANCE TRANSLATOR (ENGLISH RUSSIAN
OLGA VLASOVA FREELANCE TRANSLATOR (ENGLISH RUSSIANDRAFT ADDRESS BY IRINA BOKOVA DIRECTORGENERAL OF UNESCO
 RURAL LIBRARY SUSTAINABILITY CONTINUUM 0 AWARENESS STAGE 1
RURAL LIBRARY SUSTAINABILITY CONTINUUM 0 AWARENESS STAGE 1 2005 SZEPTEMBER 29 SCHLOTTER ILDIKÓ ILDICSBMEHU 3 GYAKORLAT MINIMÁLIS
2005 SZEPTEMBER 29 SCHLOTTER ILDIKÓ ILDICSBMEHU 3 GYAKORLAT MINIMÁLIS BLENDER FROM WIKIPEDIA THE FREE ENCYCLOPEDIA AN ELECTRIC BLENDER
BLENDER FROM WIKIPEDIA THE FREE ENCYCLOPEDIA AN ELECTRIC BLENDER PRIJAVNI OBRAZAC ZA PRISTUPANJE ORGANIZACIJE UDRUGE U RAD LOKALNOG
PRIJAVNI OBRAZAC ZA PRISTUPANJE ORGANIZACIJE UDRUGE U RAD LOKALNOGLAYOUT DO ARQUIVO TEXTO DA NOTA FISCAL VERSÃO (7)
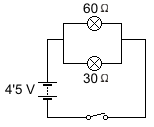 CALCULO CIRCUITOS SERIE Y PARALELO HAZ EN TU CUADERNO
CALCULO CIRCUITOS SERIE Y PARALELO HAZ EN TU CUADERNO HOW TO USE THE PTA LOGO AND TAGLINE
HOW TO USE THE PTA LOGO AND TAGLINE ¿MUTACIONES INSTITUCIONALES YO NEOLIBERALISMO?1 FRANÇOIS DUBET DURANTE LOS AÑOS
PUBLIC (INTERNAL & EXTERNAL) COUNTRY PARTNERSHIP FRAMEWORK INFORMATION NOTICE
PROPUESTAS CÉSAR CEA HONDARTZA FRAGA DANIEL GUTIERRREZ ADÁN Y
 THE BUTTERFLY HEART A STUDY GUIDE MS
THE BUTTERFLY HEART A STUDY GUIDE MS TREBALL FINAL DE GRAU TÍTOL DEL TFG TITULACIÓ GRAU
TREBALL FINAL DE GRAU TÍTOL DEL TFG TITULACIÓ GRAUEVALUATIEFORMULIER VVEKENNISKRINGBIJEENKOMST REGIO ZUID DATUMPLAATS BIJEENKOMST EINDHOVEN 19
 (1 EMPTY LINE ARIAL 10PT) (1 EMPTY LINE ARIAL
(1 EMPTY LINE ARIAL 10PT) (1 EMPTY LINE ARIAL OBČINA VITANJE GRAJSKI TRG 1 3205
OBČINA VITANJE GRAJSKI TRG 1 3205 TP SÉPARATION ET ANALYSE DES COLORANTS PRÉSENTS DANS
TP SÉPARATION ET ANALYSE DES COLORANTS PRÉSENTS DANSDIETETYKA WYKAZ OGÓLNYCH ZAGADNIEŃ ZAWODOWYCH NA EGZAMIN DYPLOMOWY 1
 DICTAMINACIÓN DE PROCEDENCIA DE NO CELEBRACION DE LICITACIÓN PÚBLICA
DICTAMINACIÓN DE PROCEDENCIA DE NO CELEBRACION DE LICITACIÓN PÚBLICA
