MAINECARE ADJUSTMENT REQUEST USE THE MAINECARE ADJUSTMENT REQUEST
MAINECARE ADJUSTMENT REQUEST USE THE MAINECARE ADJUSTMENT REQUESTMAINECAREMEDICARE PART D CLAIMS SUBMIT TO BIN 005526 PCN
NEW CITIZENSHIP AND IDENTITY REQUIREMENTS TO GET MAINECARE A
REFERRAL MAINECARE SECTION 28 REHABILITATIVE AND COMMUNITY SUPPORT SERVICES
MaineCare Adjustment Request Form
MaineCare Adjustment Request
Use the MaineCare Adjustment Request form for claim adjustments and reversals ONLY.
Ensure you provide all required information or your request will be returned.
You must complete a MaineCare Adjustment Request form for every claim that needs an adjustment or reversal with a detailed explanation of why the adjustment or reversal is needed.
You have one-hundred twenty (120) days from the date of the RA to submit a MaineCare Adjustment Request form.
The Remittance Advice (RA) and supporting documentation must be submitted with each MaineCare Adjustment Request form. Attach documentation required to complete the request. One example of documentation that may be needed to complete a request is an Explanation of Benefits (EOB) from another carrier.
You must send the original claim form. No copies will be accepted.
Prior to adjusting a claim, make sure you know why the claim paid incorrectly.
A. Original Claim Information (Complete using information from the RA):
|
1. PROVIDER NAME & CONTACT INFORMATION |
2. MEMBER NAME |
|
Name |
|
|
|
3.MEMBER ID NUMBER |
|
Phone Number |
|
|
|
4. ORIGINAL ICN NUMBER |
|
Contact Name |
|
|
|
5. REMITTANCE ADVICE DATE |
|
Pay-To NPI/API |
|
|
|
6. AMOUNT OF PAYMENT/REFUND |
|
|
|
B. Reason for Adjustment Request (Check one and give detailed explanation below):
|
Duplicate Payment |
Additional Reimbursement Requested Amount of Additional Reimbursement Requested: $ |
|
Refund Due To Payment By Primary Insurer – Please Send Primary EOB |
Refund to State Requested Amount of Reversal Requested: |
|
Billing Error |
Other |
Detailed Explanation: ______________________________________________________________________
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Signature: _________________________________________ Date: _________________________
Requests will be returned without the required information.
Mail Completed Request to:
Adjustment and Research Unit
MaineCare Services
11 State House Station, M-500
Augusta, ME 04333
Tags: adjustment request, to: adjustment, request, adjustment, mainecare
- REGLAS DEL JUEGO REGLA 1 EL TERRENO DE JUEGO
- Profesor Rndr Miloslav Pospíšil Drsc nad Hrobem Profesora Miloslava
- LIST OF SERVICE UNITS PROVIDING FEE WAIVING SUBSIDIES UNDER
- MINISTERIO DE VIVIENDA Y ASENTAMIENTOS HUMANOS CUESTIONARIO SOBRE
- MARKING GUIDELINE 0 NC…(E)(F)V SUBJECT NATIONAL CERTIFICATE (VOCATIONAL) CONSTRUCTION
- ISPARTA İL GIDA TARIM VE HAYVANCILIK MÜDÜRLÜĞÜ ŞUBE MÜDÜRÜSORUMLU
- FØR DU LESER NEDENSTÅENDE UTKAST TIL SAMARBEIDSAVTALE VÆR OPPMERKSOM
- NATIVE VEGETATION MANAGEMENT PLAN AGREEMENT BETWEEN THE NATIVE VEGETATION
- PH METRE TEKNİK ŞARTNAMESİ CIHAZ SULU ORTAMLARDA PH ÖLÇÜMÜNÜN
- WYKAZ PODMIOTÓW LECZNICZYCH W KTÓRYCH REALIZOWANE BĘDĄ SZCZEPIENIA PRZECIWKO
- C SOTO SN TFNO 948 13 02 60 FAX
- KIELCE DNIA 16 LIPCA 2015 ZNAK ZKB III 241012015
- KICY AM850 PROGRAM SCHEDULE WEEKDAYS 500 AM
- IOWA DEPARTMENT OF NATURAL RESOURCES SINGLE USE LANDFARM (PCS)
- ……………………… …………………… (IMIĘ I NAZWISKO) (MIEJSCOWOŚĆ DATA) ……………………… ………………………
- ASOCIACIÓN INDICE EVALUACIÓN DEL PROYECTO 3 EVALUACIÓN DE
- USER SETUP GUIDE THE PRINCIPAL USER (“SYSTEM ADMINISTRATOR”)
- POPIS STUDENATA PO VJEŽBOVNIM SKUPINAMA AKGOD 20202021 NEUROLOGIJA
- SLAVNOSTNI NAGOVOR PREDSEDNIKA DRŽAVNEGA SVETA MITJE BERVARJA NA OSREDNJI
- CLASIFICACIÓN DE LOS RECURSOS EN EL APRENDIZAJE DE UNA
- RELACION NO1 1 COSTOS Y GASTOS TOTALES DE
- STATE OF GEORGIA GENERAL LIABILITY INCIDENT REPORT FORM IF
- CHINESE LANGUAGE & CULTURE PROGRAMMES (NONDEGREE) ADMISSION 2017,ZHEJIANG UNIVERSITY
- JOB DESCRIPTION EXAMINATION INVIGILATOR CAUSAL PARTTIME DURING EXAM PERIODS
- LAMPIRAN A2C PERATURAN GUBERNUR NUSA TENGGARA BARAT NOMOR TAHUN
- PALERMO MEDIA PERMISSION FORM FORMA DE PERMISO DEL MÉDIUM
- EN KOMMENTAR FRA BESTYRELSEN I TEATERBUTIKKEN 2012 BESTYRELSEN ØNSKER
- ÇEVRE KOLEJİ ANAOKULLARI REHBERLİK BÜLTENİ ÇOCUKLUKTA NEGATİVİST DÖNEM ÇOCUK
- ORDU GIDA TARIM VE HAYVANCILIK İL MÜDÜRLÜĞÜ BİTKİ KORUMA
- EUROPSKA UNIJA ULAGANJE U BUDUĆNOST PRIPREMA PROJEKATA I PODRŠKA
 SCCR252 PAGE 20 E SCCR252 2ORIGINAL ENGLISH DATE NOVEMBER
SCCR252 PAGE 20 E SCCR252 2ORIGINAL ENGLISH DATE NOVEMBER LA COMA A COMA ENUMERATIVA SEPARA ELEMENTOS CORRESPONDIENTES A
LA COMA A COMA ENUMERATIVA SEPARA ELEMENTOS CORRESPONDIENTES A KLASYFIKACJA JĘZYKÓW PROGRAMOWANIA PROGRAMOWANIE TO PROCES PROJEKTOWANIA TWORZENIA TESTOWANIA
KLASYFIKACJA JĘZYKÓW PROGRAMOWANIA PROGRAMOWANIE TO PROCES PROJEKTOWANIA TWORZENIA TESTOWANIA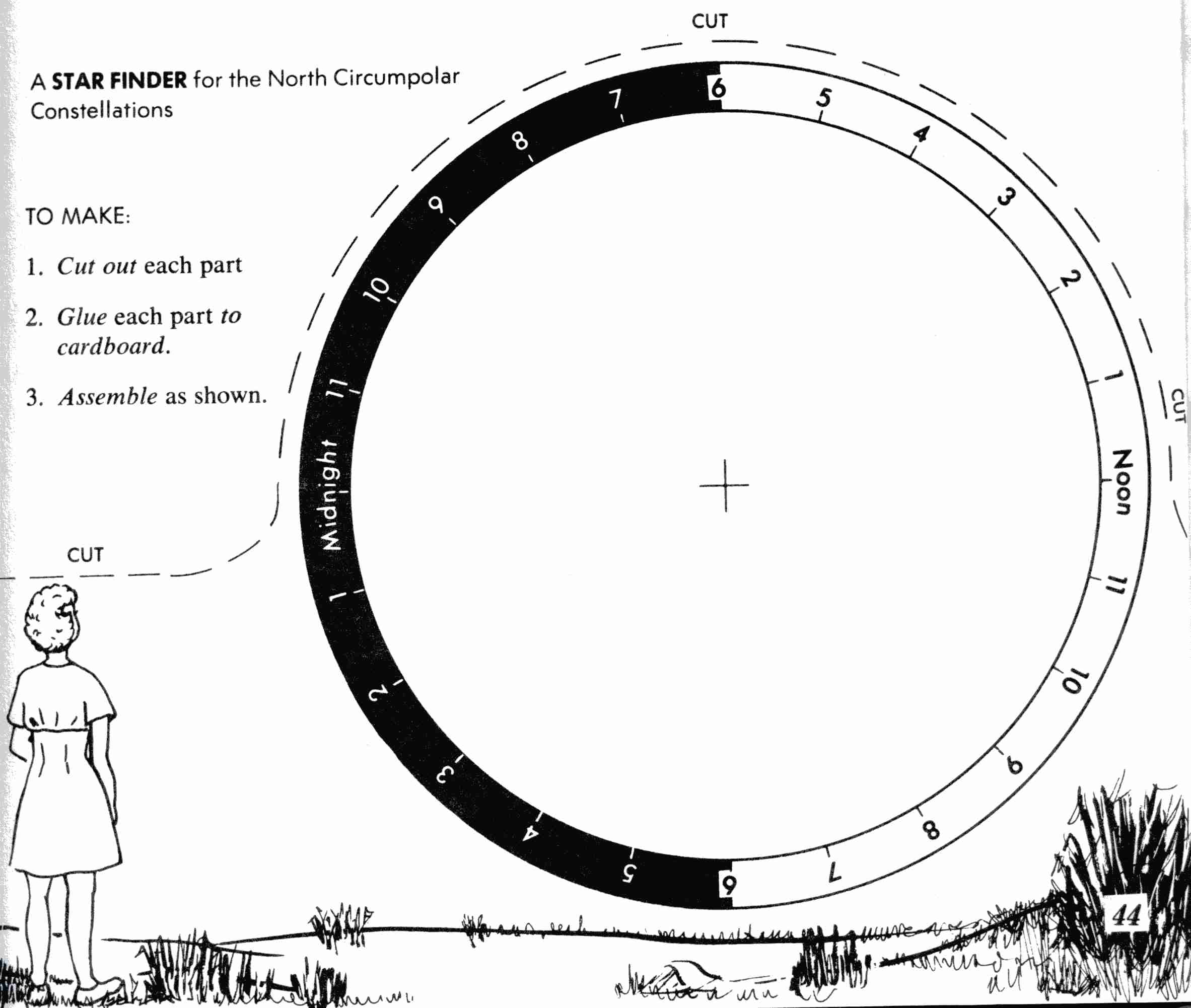 STAR FINDER ACTIVITY CREDIT THE GRAPHICS AND TEXT OF
STAR FINDER ACTIVITY CREDIT THE GRAPHICS AND TEXT OFFREEWAVE CATEGORÍA RADIO SERIAL SOLUCIÓN AREA2 COMUNICACIÓN INALÁMBRICA Y
PAŽLJIVO PROČITAJ TEKST I PODCRTAJ SVE PRIDJEVE P R
 1 ŠTA JE RELACIJA A VEZA B OPERACIJA C
1 ŠTA JE RELACIJA A VEZA B OPERACIJA CMODELO DE REPRESENTACIÓN EXCLUSIVO PARA TRÁMITES PRESENTADOS A TRAVÉS
 DEFENSA DEL CONSUMIDOR EN MENDOZA OFICINA ONLINE PARA TRÁMITE
DEFENSA DEL CONSUMIDOR EN MENDOZA OFICINA ONLINE PARA TRÁMITEDISTRIBUTED EDUCATION COORDINATION COUNCIL KAY WEISS JACK JACKSON ANDY
 ACORD DE LICENŢIERE TITLUL SETULUI DE DATE VĂ RUGĂM
ACORD DE LICENŢIERE TITLUL SETULUI DE DATE VĂ RUGĂM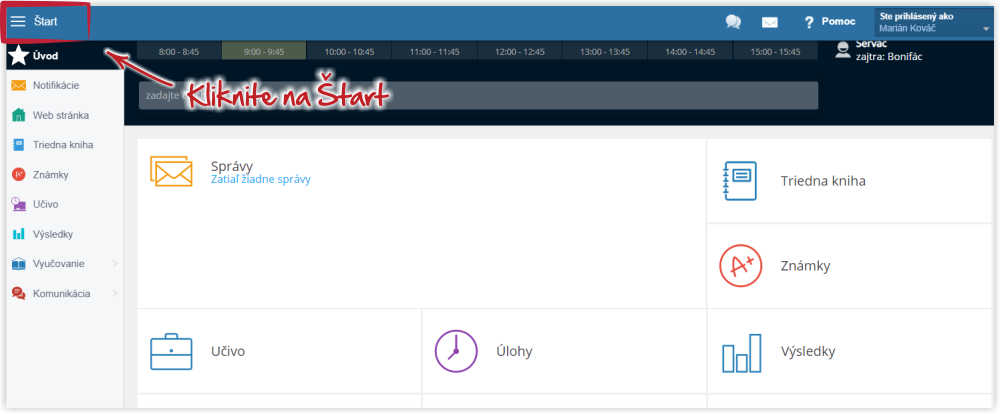 AKO VYTLAČIŤ POTVRDENIE O NÁVŠTEVE ŠKOLY PRE SVOJE DIEŤA?
AKO VYTLAČIŤ POTVRDENIE O NÁVŠTEVE ŠKOLY PRE SVOJE DIEŤA?PROJETO DE LEI MUNICIPAL Nº 0042020 DE 06 DE
ACTIVITATS SOCIOCULTURALS DE L’ASSOCIACIÓ DISCAPACITAT VISUAL CATALUNYA B1+B2+B3 GENER
 SDFJRC512009 Y ACUMULADOS JUICIOS DE REVISIÓN CONSTITUCIONAL ELECTORAL Y
SDFJRC512009 Y ACUMULADOS JUICIOS DE REVISIÓN CONSTITUCIONAL ELECTORAL Y DRUG MONOGRAPH DRUGDRUG CLASS ABILIFY DISCMELT (ARIPIPAZOLE) RAPID
DRUG MONOGRAPH DRUGDRUG CLASS ABILIFY DISCMELT (ARIPIPAZOLE) RAPID KÄNSLOSKOLAN EN UTVÄRDERING AV EN PSYKOEDUKATIV INSATS FÖR TONÅRSFLICKOR
KÄNSLOSKOLAN EN UTVÄRDERING AV EN PSYKOEDUKATIV INSATS FÖR TONÅRSFLICKOR29 SECRETARY OF STATE 2010 2011 REGULATORY AGENDA
 26 BRAINY KLASA 5 KRYTERIA OCENIANIA KRYTERIA OCENIANIA PROPONOWANE
26 BRAINY KLASA 5 KRYTERIA OCENIANIA KRYTERIA OCENIANIA PROPONOWANELET’S WRITE! JOURNAL TOPICS DIRECTIONS PLEASE COMPLETE A JOURNAL
