PATIENT INFORMATION COMMON FEMORAL ENDARTERECTOMY THE OPERATION EXPLAINED
ISSUE 4 DEAR PATIENT WELCOME TOPATIENT DATA FORM FOR ADULTS (AGED 15
PATIENT GUIDE TO ACL INJURIES WHAT IS
PATIENT HISTORY NAME AGE DATE 1 DESCRIBE
PATIENT ID NUMBER PATIENT NAME INFORMED CONSENT
PULMONARY REHABILITATION COMMUNITY REFERRAL PATIENT NAME………………………………NHS
Patient Information –

Patient Information
Common femoral endarterectomy - The Operation Explained
1. Why do I need the operation?
There is a blockage of the artery supplying your leg and the circulation of blood to your leg is reduced. The operation is to remove the fatty deposits (plaque) surgically, through an opening in the artery. This will improve the circulation to your leg.
2. Before your operation
Before surgery, there are a number of tests that may need to be done. These are of two types:
1. Tests of fitness and suitability are normally done before a decision to operate is made. They normally include: blood tests, ECG (electrical tracing of the heart), an ultrasound scan of the blocked artery and/or an X-ray of the arteries (arteriogram).
2. Immediate pre-operative tests include: blood tests, another ECG and completing the paperwork. These tests are usually completed at a pre-admission visit to the hospital a few days before your operation. Occasionally, they are done when you are admitted to hospital for the operation.
3. Coming into hospital
Please bring with you all the medications that you are currently taking. You will be admitted to your bed by one of the nurses who will also complete your nursing record.
You will be visited by the Surgeon who will be performing your operation and also by the doctor who will give you the anaesthetic. Your operation may be performed by a different Vascular Consultant to the one who saw you in clinic.
Physiotherapists and Intensive Care staff may also visit to give you information about your post-operative care. If you have any questions regarding the operation please ask the Doctors.
4. The Anaesthetic
The first part of the operation involves giving you an anaesthetic. The operation can be done with you asleep, or awake:
If you go to sleep, a tiny needle is placed in the back of your hand. The anaesthetic is injected through the needle and you will be asleep within a few seconds.
If you are to be awake, you will have a small tube placed in your back. This may be a spinal or an epidural anaesthetic
A spinal anaesthetic stops you from feeling anything from the waist downward on the operation side. The leg is paralysed. This anaesthetic lasts for about 2-2½ hours.
An epidural again stops you from feeling anything from the waist downwards, and affects both legs. There is no paralysis however. The epidural is like a drip and can stay in for several days to provide post-operative pain relief.
A tube (catheter) may be inserted into your bladder to drain your urine. The catheter is essential if you have either the spinal or epidural anaesthetic.
For all three options, a drip is placed into a vein in your forearm to give you some fluids during and following surgery.
5. The Operation
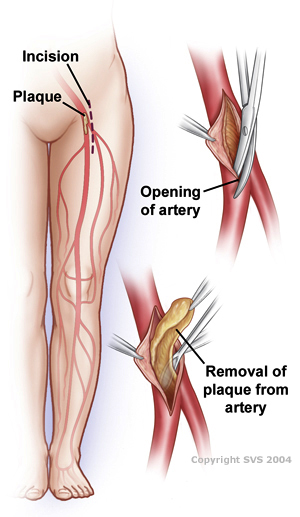
Normally a cut about 10cm (4inches) long is made in the groin to expose the main artery (Common Femoral Artery) supplying the leg.
The plaque is removed and the artery is closed using a patch of vein or synthetic material.
At the end of the operation, the wounds are all closed either with dissolving stitches, which do not need to be removed, or with a non-dissolving stitch or metal clips which will normally be removed after about ten days.
6. After the operation
After your operation you will be given fluids by a drip in one of your veins until you are well enough to sit up and take fluids and food by mouth.
The nurses and doctors will try and keep you free of pain by giving pain killers by injection, via the epidural tube in your back or by a machine that you are able to control yourself by pressing a button (PCA – patient controlled analgesia).
Within a day or so, the drip, epidural and bladder catheter will be removed.
You will become gradually more mobile until you are fit enough to go home.
You may be visited by the physiotherapists after your operation. They will help you with your breathing to prevent you developing a chest infection and with your mobilisation to get you walking again.
7. Going home
After this type of surgery, patients normally return home about 5 days after the operation.
If your stitches or clips are the type that needs removing, this is usually done whilst you are still in hospital. If not, we will arrange for your GP’s practice or district nurse to remove them and check your wound.
You may feel tired for some weeks after the operation but this should gradually improve as time goes by.
Regular exercise such as a short walk combined with rest is recommended for the first few weeks following surgery followed by a gradual return to your normal activity.
Driving: You will be safe to drive when you are able to perform an emergency stop. This will normally be 2-4 weeks after surgery, but if in doubt check with your own doctor.
Bathing: Once your wound is dry you may bathe or shower as normal.
Work: You should be able to return to work within 6-12 weeks of surgery. We will provide you with a sick note but if you need longer off work, please see your GP.
Medicines: You will usually be sent home on a small dose of aspirin if you were not already taking it. This is to make the blood less sticky. If you are unable to tolerate aspirin, an alternative drug may be prescribed.
8. Complications
Thrombosis and embolism (clotting of the artery) at the surgical site or beyond it. If this occurs, it is usually necessary to perform a second operation to re-open the artery.
Wound infection: Wounds sometimes become infected and this may need treatment with antibiotics. Bad infections are rare. Occasionally, the wound may need to be cleaned out under anaesthetic.
Fluid in the wound: Occasionally, the wound may fill with fluid (lymph). This may be clear but is often blood stained. It normally settles in time but may require suction (aspiration) to help remove the fluid.
Skin sensation: You may have patches of numbness around the wound due to the inevitable cutting of small nerves to the skin. This usually gets better within a few months.
Chest infections: These can occur following this type of surgery, particularly in smokers, and may require treatment with antibiotics and physiotherapy.
Major complications: As with any major operation there is a small risk of you having a medical complication such as a heart attack, stroke, kidney failure, chest problems, loss of circulation in the legs or bowel or infection in the artificial artery. Each of these is rare, but overall it does mean that some patients may have a fatal complication from their operation. For most patients this risk is about 5% - in other words 95 in every 100 patients will make a full recovery from the operation. The doctors and nurses will try to prevent these complications and to deal with them rapidly if they occur.
9. What can I do to help myself?
If you were previously a smoker, you must make a sincere and determined effort to stop completely. Continued smoking will cause further damage to your arteries. It is also likely to jeopardise the success of any surgical operation carried out and to make recovery more difficult.
Why not take this opportunity to consult your own doctor or the practice nursing staff to seek professional help in giving up the addiction?
Further help is available locally from the
Smoking Advice Service Tel: 01752 314040 www.smokingadvice.com
General health measures such as reducing weight, a low fat diet and regular exercise are also important. If you develop sudden pain or numbness in the leg which does not get better within a few hours, then contact your GP or the hospital immediately.
Vascular patients are known to be at increased risk of heart attack and stroke. You should talk to your doctor about taking low dose Aspirin or an alternative anti-platelet agent in order to thin the blood and to help reduce the likelihood of developing a heart attack or stroke. In addition, your doctor may advise taking a statin, which will reduce your cholesterol level, further decreasing these risks.

Version November 2014
|
VASCULAR SURGICAL UNIT
SURGICAL DIRECTORATE
PLYMOUTH HOSPITALS NHS TRUST DERRIFORD HOSPITAL PL6 8DH TEL 0845 155 8155
|
CONSULTANT VASCULAR SURGEON & LEAD CLINICIAN Surgeon Commander Cris Parry RN
|
Secretary: 01752 431809 |
|
CONSULTANT VASCULAR & TRANSPLANT SURGEON Mr Jamie Barwell |
Secretary: 01752 431809
|
|
|
CONSULTANT VASCULAR SURGEON Mr Francis Dix |
Secretary: 01752 431822
|
|
|
CONSULTANT VASCULAR SURGEON Miss Catherine Western |
Secretary: 01752 431805
|
|
|
CONSULTANT VASCULAR SURGEON Mr Devender Mittapalli |
Secretary: 01752 431822 |
|
|
CONSULTANT VASCULAR SURGEON Lt Col Robert Faulconer |
Secretary: 01752 431805 |
|
|
VASCULAR SCIENTISTS Mrs J George Mr A Ellison Mr R Craven
|
01752 439228
|
|
|
VASCULAR NURSE SPECIALIST Mr Alan Elstone |
01752 431805
|
|
|
MATRON Judy Frame
|
01752 431847 |
Patient information –Common femoral endarterectomy
TREAT PATIENTS IN A CLEAN AND SAFE ENVIRONMENT
0 INTERMITTENT POSITIVEPRESSURE BREATHING EFFECTS IN PATIENTS WITH HIGH
1 ASSIST IN THE PREPARATION OF PATIENTS FOR OPERATIVE
Tags: common femoral, endarterectomy, common, femoral, explained, information, patient, operation
- DDª COMO RESPONSABLE DEL SERVICIODEPARTAMENTO AUTORIZA A DDª
- NA OSNOVU ČLANA 1 ZAKONA O JAVNIM NABAVKAMA BOSNE
- USECHE 4 IMPORTANCIA DEL LECTOR EN UN ENFOQUE DESDE
- ENGINEERING SPECIFICATIONS TRS 371 FULLHEIGHT TURNSTILE – SINGLE PASSAGEWAY
- LA ESCUELA DEL HAMBRE ANÓNIMO JAPONÉS ESTA HISTORIA ACONTECE
- NZQA DRAFT UNIT STANDARD RU01 VERSION 1 PAGE 6
- DERS BİLGİ FORMU DERSİN ADI MESLEKİ MATEMATİK BÖLÜM MUHASEBE
- TITLE RECURRENCE RATES OF BIPOLAR DISORDER DURING THE POSTPARTUM
- SPS STRATEGY ON THE MANAGEMENT OF DRUG MISUSE PATHWAYS
- RETOS ACTUALES EN PSICOTERAPIA PSICOANALÍTICA CON NIÑOS Y ADOLESCENTES
- Ðïࡱáþÿ ¦¨þÿÿÿ¤¥¥á` Ø¿kbjbjæx87æx87 x84íx84íkÿÿÿÿÿÿ¤øøøøøøø 4444 ¶xxxxx333¡££££££øhhçø33333çøøxxûüx85x85x853øxøx¡x853¡x85x85øøx85xl Ð4x85b¡
- PERFIL DOCENTE ESTUDIO DEL PERFIL DOCENTE DE LA ESCUELA
- GUIDANCE WHAT EQUALITY LAW MEANS FOR YOU AS A
- P LATAFORMA POR LA DESPOLITIZACIÓN Y LA INDEPENDENCIA JUDICIAL
- NYISO TARIFFS OPEN ACCESS TRANSMISSION TARIFF (OATT)
- DEWHURST LAB MANUAL NEW MEMBER GUIDE LAST UPDATE
- AUGUST 2019 815 BEECH STREET MANCHESTER NH 03104 6036697361
- ISOIEC 100211 DAM 1 MESSAGE STORE EXTENSIONS AND
- INSTRUCTIONS FOR REGRESSION PROJECT WITH POINT VALUES (
- BIOTECHNOLOGIC METHODS AND TESTS FOR IMPROVING THE SALMONELLA MONITORING
- FERMA OLDAR ALEKSANDRA DĘBSKA SOKOŁÓW 15 MAJA 2012 R
- ЈКП „ТРЖНИЦА“ НИШ ЂУКЕ ДИНИЋ БР 4 НА
- KATOWICE DNIA 11032015 R PSII0003 2015AK SZANOWNY PAN PIOTR
- ZAHTJEV ZA SUBVENCIJU ZA NABAVU SADNICA JAGODA U OPĆINI
- Bruneicambridge gce a& as Level June 2008 Bn105 Maktab
- AYUNTAMIENTO DE BARBASTRO ANEXO V RELACIÓN DEL GASTO TOTAL
- ( 288 ) DAV DEGREE COLLEGE VARANASI DR
- FORMAT A1 NOMOR JAKARTA …………………… LAMPIRAN
- LISTA DE DIÁLOGOS “TRÁNSITO” IDIOMA ESPAÑOL RAQUEL PABLO PABLO…
- ARVEAVGIFTEN I STØPESKJEEN (PUBLISERT I SKATTERETT NR 3 2000)
GENERIC JOB DESCRIPTON TEACHING ASSISTANT LEVEL 3 WITH SPECIALISM
NAZWA ZAJĘĆ GENETYKA POPULACJI ECTS 6 NAZWA ZAJĘĆ W
 DEPAUW UNIVERSITY LACROSSE 2015 INTRODUCTION THIS MANUAL SHOULD SERVE
DEPAUW UNIVERSITY LACROSSE 2015 INTRODUCTION THIS MANUAL SHOULD SERVEGRIGLIA DI VALUTAZIONE PPT GEOGRAFIA STUDENTE CLASSE 1^ A
ÜBER EINIGE ANGEBOTE FREUT MAN SICH ANDERE BRAUCHT MAN
´ ORDENANZA DEL PRECIO PÚBLICO NUM 2 REGULADORA DEL
PŘIPOMÍNKOVACÍ FORMULÁŘ K VÝSTUPŮM Z MAPOVÁNÍ SOCIÁLNÍ SITUACE NA
GSPSNEEC196ADD10 PAGE 0 ORGANIZACIÓN MUNDIAL DEL COMERCIO GSPSNEEC196ADD10 28
 NATIONAL INSURANCE COMPANY LIMITED TENDER DOCUMENT FOR SELECTION OF
NATIONAL INSURANCE COMPANY LIMITED TENDER DOCUMENT FOR SELECTION OF 2015 GLOBAL COUNCIL 1215 APRIL 2015 GRAND
2015 GLOBAL COUNCIL 1215 APRIL 2015 GRAND ORDEN DE ELEMENTOS PROGRAMADOS ESTE DOCUMENTO DEBE SER REENVIADO
ORDEN DE ELEMENTOS PROGRAMADOS ESTE DOCUMENTO DEBE SER REENVIADO PRÉFET DE PARIS DIRECTION DÉPARTEMENTALE DE LA COHÉSION SOCIALE
PRÉFET DE PARIS DIRECTION DÉPARTEMENTALE DE LA COHÉSION SOCIALEPOUDARKI IZ 11 REDNE SEJE OS OBČINE ŠENTJUR SVETNIKI
PREGUNTA ESCRITA E013507 DE ERIK MEIJER (GUENGL) A LA
PRINTEMPS ARABE ART CONTEMPORAIN QUAND DES ARTISTES ARABES
 EXPERTA INDEPENDIENTE SOBRE LA CUESTIÓN DE LAS OBLIGACIONES DE
EXPERTA INDEPENDIENTE SOBRE LA CUESTIÓN DE LAS OBLIGACIONES DE SENATE NO 2843 STATE OF NEW JERSEY 216TH LEGISLATURE
SENATE NO 2843 STATE OF NEW JERSEY 216TH LEGISLATUREDEPARTMENT OF MATHEMATICS ANNUAL EVALUATION GUIDELINES (APPROVED BY FACULTY
 SOLICITUD DE DUPLICADO DE LIBRO DE FAMILIA EN PARÍS
SOLICITUD DE DUPLICADO DE LIBRO DE FAMILIA EN PARÍSQS3KOVIUDIRRT32018 DETALJNI IZVEDBENI PLAN KOLEGIJA 1 OPĆE INFORMACIJE 1
